

Volume 13, Issue 1 (1-2024)
JCHR 2024, 13(1): 1-7 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Thapa G, Dowerah S. Prevalence of Anemia in Pregnant Women and Its Associated Socioeconomic Factors. JCHR 2024; 13 (1) :1-7
URL: http://jhr.ssu.ac.ir/article-1-975-en.html
URL: http://jhr.ssu.ac.ir/article-1-975-en.html



1- Department of Community Medicine, Tinsukia Medical College, Tinsukia, India
2- Department of Pathology, Tinsukia Medical College, Tinsukia, India ,swagatadowerah@gmail.com
2- Department of Pathology, Tinsukia Medical College, Tinsukia, India ,
Full-Text [PDF 543 kb]
(647 Downloads)
| Abstract (HTML) (886 Views)
How to cite this paper:
Introduction
Results

Table 2.Mean Hb levels of the subjects in different trimesters

Table 3. Distribution of the subjects according to IFA consumption

Table 4.The relationship between the type of family and the mean Hb levels

Table 5. The relationship between the socio-economic status of the subjects and their mean Hb levels

Table 6. The relationship between the educational qualification of the subjects and their mean Hb levels
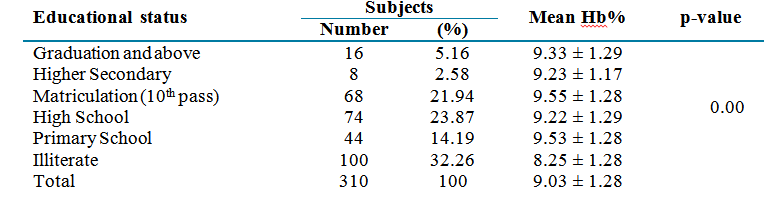
Table 7. The relationship between the type of occupation of the subjects and their mean Hb levels

Table 8.Therelationship between tobacco consumption in the subjects and their mean Hb levels

Table 9. The relationship between betel nut intake in the subjects and their mean Hb levels

Conclusion
Acknowledgment
References
Full-Text: (762 Views)
| Prevalence of Anemia in Pregnant Women and Its Associated Socioeconomic Factors |

- Department of Community Medicine, Tinsukia Medical College, Tinsukia, India
- Department of Pathology, Tinsukia Medical College, Tinsukia, India
| ARTICLE INFO | ABSTRACT | |
| Original Article Received: 12 Feb 2023 Accepted: 28 Jun 2023 |
Background: Anemia during pregnancy is an important public health problem, in developing countries. This community based study was conducted in Northeast India to study the prevalence of anemia along with the associated socioeconomic factors.
Methods: The present one-year cross sectional study was carried out in the selected villages under Lahowal Block of Dibrugarh District and the relevant data was collected in a pre-designed and pre-tested proforma by house to house interviews. The sample size was calculated 310. Clinical examination was done and haemoglobin estimation was performed using Sahli’s acid hematin method. Data were analyzed in Microsoft Excel using percentage, range, t-test and ANOVA; wherever applicable. A significance level of 5% was taken with 95% confidence interval
Results: Anemia was seen in 89.68% of the subjects. The highest mean hemoglobin (Hb) level was observed in the 1st trimester subjects (9.14 gm/dl), while the lowest mean Hb-level was observed in the 3rd trimester subjects (8.90 gm/dl). A significant difference was observed between the mean Hb-levels of the study subjects belonging to nuclear families and joint families, subjects belonging to different socio-economic status, different levels of education, different professions, those consuming tobacco and those not consuming tobacco, and those consuming betel nut and not consuming betel nut. Conclusion: There was a high prevalence of anemia in pregnancy which was related to the socioeconomic status, occupational status, level of education, type of family, and personal habits in these women. Keyword: Anemia, Pregnancy, Hemoglobin |
|
Corresponding Author: Swagata Dowerah swagatadowerah@gmail.com |
Thapa G, Dowerah S. Prevalence of Anemia in Pregnant Women and Its Associated Socioeconomic Factors. J Community Health Research. 2024; 13(1): 1-7.
Introduction
Anemia during pregnancy, defined by the World Health Organization (WHO) as hemoglobin (Hb) concentration of less than 11 g/dl, is an important public health problem; more commonly in the developing countries (1). Anemia during pregnancy was found to have the highest prevalence in Sub-Saharan Africa (SSA) (57%). A slightly lower prevalence (48%) was in Southeast Asia, and the lowest prevalence (24.1%) was found among pregnant women in South America (2). Notable causes of anemia in developing countries include less than adequate intake and poor absorption of iron, malarial infection, hookworm infestation, diarrheal diseases, HIV/AIDS, diseases of red blood cells like sickle cell anemia and thalassemia, blood loss during labor, and pregnancies at close intervals(2) (1, 3).Since there is an increased requirement of iron among pregnant women, factors like early onset of childbearing, a high number of births, short intervals between births, and poor access to antenatal care and nutritional supplementation contribute to anemia and poor pregnancy outcome in these women (4). Iron deficiency is the most significant cause of anemia in this population and early institution of iron therapy could considerably reduce the burden of anemia in these women, thereby improving fetal outcome. According to the National Family Health Survey 4 (NFHS-4) data, India has a high prevalence of anemia in pregnancy (50% in 2015-2016) with only a minimal 8% reduction from 2005 to 2006(NFHS-3) (3, 4). In Assam, one of the major states of Northeast India, the prevalence of anemia among pregnant women was 54% in 2019-2020 (NFHS-5), while it was 44.8% in 2015-2016 (NFHS4) (5). This shows a rise in the problem of anemia among the pregnant population in the state and is an indicator of under-nutrition in this population. Therefore, the present community based study was conducted on the prevalence of anemia and its associated socioeconomic factors in a district of North east India.
Method
This cross sectional studywas carried out in the selected villages under LahowalBlock of Dibrugarh. The Dibrugarh district of Assam is divided into 6 blocks, and 1362 villages. Among the 6 blocks, Lahowal block was selected randomly for the study. All pregnant women aged 15-45 years in the selected villages were studied for a one-year period. Cases were selected by a multistage sampling device and the calculated sample size was 310.
Inclusion criteria: Pregnant women were included in the study by the following inclusion criteria:
1. Willing to give consent to participate in the study.
2. Have resided in the identified village, for a period of at least 1 year prior to the date of the interview.
Exclusion criteria:
1. Not willing to participate in the study.
2. Those pregnant women who were not available for interview even after 2 visits to their houses.
Data collection: The selected villages were visited on predetermined dates and the relevant
data was collected in a pre-designed and
pre-tested proforma by house to house interviews.Demographic variables such as age, gravida, type of family, caste, educational qualification, occupation were noted. To evaluate the socioeconomic status, Modified BG Prasad classification was used. Clinical examination was done and Hb estimation was performed using Sahli’s acid hematin method.
Analysis: Analysis of data was done using percentage, range, t-test and ANOVA. The data were presented by calculating percentage and range and the level of significance was determined using t-test and ANOVA.
The procedures followed were in accordance with the institutional ethical standards [No. AMC/EC/12638]. Informed consent was taken from the participants prior to the study.
Method
This cross sectional studywas carried out in the selected villages under LahowalBlock of Dibrugarh. The Dibrugarh district of Assam is divided into 6 blocks, and 1362 villages. Among the 6 blocks, Lahowal block was selected randomly for the study. All pregnant women aged 15-45 years in the selected villages were studied for a one-year period. Cases were selected by a multistage sampling device and the calculated sample size was 310.
Inclusion criteria: Pregnant women were included in the study by the following inclusion criteria:
1. Willing to give consent to participate in the study.
2. Have resided in the identified village, for a period of at least 1 year prior to the date of the interview.
Exclusion criteria:
1. Not willing to participate in the study.
2. Those pregnant women who were not available for interview even after 2 visits to their houses.
Data collection: The selected villages were visited on predetermined dates and the relevant
data was collected in a pre-designed and
pre-tested proforma by house to house interviews.Demographic variables such as age, gravida, type of family, caste, educational qualification, occupation were noted. To evaluate the socioeconomic status, Modified BG Prasad classification was used. Clinical examination was done and Hb estimation was performed using Sahli’s acid hematin method.
Analysis: Analysis of data was done using percentage, range, t-test and ANOVA. The data were presented by calculating percentage and range and the level of significance was determined using t-test and ANOVA.
The procedures followed were in accordance with the institutional ethical standards [No. AMC/EC/12638]. Informed consent was taken from the participants prior to the study.
Results
A total of 310 pregnant women in the age group of 15-45 years were selected and included in the study. Anemia was seen in 89.68% of the subjects, 2.9% of whom had severe anemia, while 59% had moderate anemia and 38% had mild anemia (Table 1). Among the subjects, the highest mean Hb-level was observed in the 1st trimester subjects (9.14 gm/dl), while the lowest mean Hb-level was observed in the 3rd trimester subjects (8.90 gm/dl) (Table 2). Moreover, 8.6% of the 2nd trimester study subjectsand3.64% of the 3rd trimester subjects did not consume IFA (Table 3). A significant difference was observed between the mean Hb levels of the study subjects belonging to nuclear families and joint families (Table 4).There was a significant difference between the mean Hb levels of the study subjects belonging to different socio-economic status (Table 5). It was seen that Hb levels were much lower among the illiterate pregnant women compared to the educated pregnant women. A significant difference was found between the mean Hblevels of the subjects with different levels of education (Table 6). There was a significant difference between the mean Hb levels of the study subjects belonging to different professions (Table 7). However, no significant difference was observed between the mean Hb levels of the subjects belonging to different castes. There was a significant difference between the mean Hb levels of the subjects consuming tobacco and those not consuming tobacco. A significant difference was also observed between the mean Hb levels of the subjects consuming betel nut and not consuming betel nut (Tables 8 and 9).
In the present study conducted on 310 pregnant women over a period of 1 year, 41.94% were primigravida and 58.06% were multigravida. The majority of the pregnant women (41.29%) were in the age group of 23-26 years, followed by 38.71% in the age group of 19-22 years. Furthermore, 25.81% of the study subjects belonged to nuclear families and 74.19% were from joint families.
In the present study conducted on 310 pregnant women over a period of 1 year, 41.94% were primigravida and 58.06% were multigravida. The majority of the pregnant women (41.29%) were in the age group of 23-26 years, followed by 38.71% in the age group of 19-22 years. Furthermore, 25.81% of the study subjects belonged to nuclear families and 74.19% were from joint families.
Table 1.Distribution of the subjects according to the severity of anemia
Table 2.Mean Hb levels of the subjects in different trimesters
Table 3. Distribution of the subjects according to IFA consumption
Table 4.The relationship between the type of family and the mean Hb levels
Table 5. The relationship between the socio-economic status of the subjects and their mean Hb levels
Table 6. The relationship between the educational qualification of the subjects and their mean Hb levels
Table 7. The relationship between the type of occupation of the subjects and their mean Hb levels
Table 8.Therelationship between tobacco consumption in the subjects and their mean Hb levels
Table 9. The relationship between betel nut intake in the subjects and their mean Hb levels
Discussion
A high prevalence of anemia (89.68%) was observed in the current study. Saxena, et al. (11) who conducted their study on anemia in pregnant women observed the prevalence of anemia to be 38%, while Suryanarayana, et al. (12) reported the prevalence to be 62.3% in their study. Other studies have reported the anemia prevalence of 82.9% (Viveki, et al), 84.9 % (Totega, et al), and 96.6% (13, 14, 15).
The majority of the pregnant women (41.29%) were in the age group of 23-26 years followed by 38.71% in the age group of 19-22 years. In a study by Rajamouli, J., et al. (16), most of the cases were in the age group of 20 to 29 years (77.3%), while in a study in Aurangabad city, India, by Pushpa, O., Lokare, 87.2% of the subjects were in the age group of 20-30 years (17); 25.81% of the total study subjects belonged to nuclear families and 74.19% were from joint families. These findings correlate with the study by Sahoo, et al. (18), in which 26.7% of the respondents belonged to nuclear families and 73.3% belonged to joint families. In the same study, on nutritional status of pregnant women in rural Balasore district, Orissa, in 2006, it was observed that 45.7% belonged to middle caste. However, in the present study, 76.13% of the subjects belonged to other backward castes. In a study conducted by Siddiqui, et al. (19), women belonging to scheduled caste and scheduled tribe had a significantly higher burden of anemia than other backward classes, which is in line with the present study
In the present study, out of 310 pregnant women, 49.03% were from class IV (Modified BG Prasad) and 23.23% were from class V (Modified BG Prasad). Thus, majority of pregnant women suffering from anemia came from the lower socioeconomic strata of the population. This finding has been supported by the studies of Sarala V et al. and Ahmad N et al., who noted that anemia was more common in lower socioeconomic strata of women (20,21). K, Kavitha in her study on nutritional status of pregnant women in rural area of Tamil Nadu in 2011 also observed that 70% of the study population had a monthly income ranging from Rs. 2000 to Rs. 4000 (22). This emphasizes the fact that among the poorer section of the society, due to financial constraints, these women do not get adequate nutrition during pregnancy and thus suffer from anemia.
In the present study, a statistically significant difference was seen between the mean Hb values of the subjects in relation to their level of education. Moreover, 76.13% of the subjects were housewives and 18.71% comprised of tea garden female workers. Sahoo et al. (18) stated that majority of the cases were house wives (93.3%) and the remaining (6.7%) were self-dependent. Rajamouli et al. also noted a high prevalence of (96.8%) anemia among housewives and agricultural labourers compared with employees, only 3.2% of whom were anemic (16). A statistically significant difference was observed among the mean Hb values and the type of occupation in the current study with mean Hb levels much lower in the housewives and tea garden workers. This could partly be due to the lower income in these families.
In the present study, a statistically significant difference was seen between the mean Hb values of the subjects in relation to their level of education. Moreover, 76.13% of the subjects were housewives and 18.71% comprised of tea garden female workers. Sahoo et al. (18) stated that majority of the cases were house wives (93.3%) and the remaining (6.7%) were self-dependent. Rajamouli et al. also noted a high prevalence of (96.8%) anemia among housewives and agricultural labourers compared with employees, only 3.2% of whom were anemic (16). A statistically significant difference was observed among the mean Hb values and the type of occupation in the current study with mean Hb levels much lower in the housewives and tea garden workers. This could partly be due to the lower income in these families.
In the present study, the mean 24-hour caloric intake of all pregnant women irrespective of their duration of pregnancy was found to be 1151.82 ± 235.31 kcal. It was less than the RDA (2525 kcal/24hours) (Recommended Dietary Allowance). K. Kavitha in her study observed that the mean caloric intake of the study population was 2067. 45 kcal/day; lower than the RDA, while Sahoo et al. observed that the mean 24-hour caloric intake was 2181.92 ± 311.21 kcal, which was also less than the RDA (18, 22). Gautam VP, et al. who carried out a study on dietary aspects of pregnant women in rural areas of northern India in 2008 observed that the mean caloric intake of the study subjects was less than the RDA in all (100%) of pregnant women who participated in the study (23). The mean caloric intake of the present study subjects was not only less than the RDA, but was also found to be less than the mean caloric intake of other study subjects sited above. This difference in the mean caloric intake of the subjects in comparison to other studies may be due to different dietary and socio-cultural habits and also because of difference in the geographical location.
In the current study, the mean Hb levels of the 1st trimester study subjects was higher than that of the 2nd trimester women and the mean Hb levels further decreased in the 3rd trimester of pregnancy. However, Subarnalata, Sahoo and Basumati, Panda in their study on nutritional status of pregnant women of some villages in Balasore, Orissa, reported that the mean Hb-levels increased from the 1st to 3rd trimester of pregnancy (18).
A significant difference in the mean Hb-levels of the study subjects was found in relation to the type of family (p < 0.05), socio-economic status (p < 0.05), educational status (p < 0.05), type of occupation (p < 0.05), betel nuts with lime consumption (p < 0.05), and tobacco intake (p <0.05). From the overall results of the study, it could be inferred that the type of family, socioeconomic status, educational status, type of occupation, consumption of betel nut with lime, and tobacco intake all contributed to the burden of anemia in this population.
Although most of the participants belonged to other backward classes, the difference in the mean Hb-levels of the study subjects was not significant (p > 0.05) for the caste of the person.
A significant difference in the mean Hb-levels of the study subjects was found in relation to the type of family (p < 0.05), socio-economic status (p < 0.05), educational status (p < 0.05), type of occupation (p < 0.05), betel nuts with lime consumption (p < 0.05), and tobacco intake (p <0.05). From the overall results of the study, it could be inferred that the type of family, socioeconomic status, educational status, type of occupation, consumption of betel nut with lime, and tobacco intake all contributed to the burden of anemia in this population.
Although most of the participants belonged to other backward classes, the difference in the mean Hb-levels of the study subjects was not significant (p > 0.05) for the caste of the person.
Conclusion
There was a high prevalence of anemia among the pregnant women in the study population, which was related to the socioeconomic status, occupational status, level of education, type of family, personal habits like consumption of betel nut and tobacco in these women. Public health measures like screening programs for anemia, conducting awareness campaigns, providing access to proper antenatal care, food fortification, iron and folic acid supplementation, spacing of pregnancies and change of habits in these women would go a long way towards reducing the burden of anemia in these women, thereby improving pregnancy outcomes.
Acknowledgment
The authors would like to thank Department of Community Medicine, Assam Medical College for their support.
Conflicts of interest
The authors declare that there is no conflict of interest.
Funding
None
Ethical considerations
The study was carried out in accordance with the institutional ethical standards and the Helsinki Declaration. Informed consent was taken and the data was de-identified. Permission from the institutional ethical committee was taken before carrying out the study.
Code of Ethics
No. AMC/EC/12638
Authors’ contributions
G. T., data collection and analyzed the data; S. D., review of literature and manuscript preparation. Manuscript was reviewed by both authors.
Open Access Policy
JCHR does not charge readers and their institution for access to its papers. Full text download of all new and archived papers are free of charge.
Conflicts of interest
The authors declare that there is no conflict of interest.
Funding
None
Ethical considerations
The study was carried out in accordance with the institutional ethical standards and the Helsinki Declaration. Informed consent was taken and the data was de-identified. Permission from the institutional ethical committee was taken before carrying out the study.
Code of Ethics
No. AMC/EC/12638
Authors’ contributions
G. T., data collection and analyzed the data; S. D., review of literature and manuscript preparation. Manuscript was reviewed by both authors.
Open Access Policy
JCHR does not charge readers and their institution for access to its papers. Full text download of all new and archived papers are free of charge.
References
1. World Health Organization. Iron defciency anaemia: assessment, prevention and control: a guide for programme managers; 2001.
2. World Health Organization. Worldwide prevalence of anaemia 1993-2005: WHO global database on anaemia; 2008.
3. Tolentino K, Friedman JF. An update on anemia in less developed countries. The American journal of tropical medicine and hygiene. 2007; 77(1): 44-51.
4. Balarajan Y, Ramakrishnan U, Özaltin E, et al. Anaemia in low-income and middle-income countries. The lancet. 2011; 378(9809): 2123-35.
5. Crawley J. Reducing the burden of anemia in infants and young children in malaria-endemic countries of Africa: from evidence to action. The Intolerable Burden of Malaria II: What's New, What's Needed: Supplement to Volume 71 (2) of the American Journal of Tropical Medicine and Hygiene. 2004; 71(Suppl): 25-34.
6. Maskey M, Jha N, Poudel SI, et al. Anemia in pregnancy and its associated factors: A study from Eastern Nepal. Nepal journal of epidemiology. 2014; 4(4): 386-92.
7. Abay A, Yalew HW, Tariku A, et al. Determinants of prenatal anemia in Ethiopia. Archives of Public Health. 2017; 75: 1-0.
8. International Institute for Population Sciences (IIPS) and ICF.Assam: NFHS4 (2015-16). [Online]; 2015. Available at: URL: http://rchiips.org/NFHS/NFHS-4Reports/Assam.pdf..
9. Nternational Institute for Population Sciences (IIPS) and ICF. Assam:NFHS3 (2005 -06). [Online]; 2006. Available at: URL: http://rchiips.org/nfhs/pdf/Assam.pdf.
10. International Institute for Population Sciences (IIPS) and ICF.Assam: NFHS5 (2019-20). [Online]; 2020. Available at: URL: https://nhm.assam.gov.in/sites/default/files/swf_utility_folder/departments/nhm_lipl_in_oid_6/ menu/document/factsheet_as.pdf.
11. Saxena V, Srivastava VK, Idris MZ, et al. Nutritional status of rural pregnant women. Indian Journal of community medicine. 2000; 25(3): 104-7.
12. Suryanarayana R, Chandrappa M, Santhuram AN, et al. Prospective study on prevalence of anemia of pregnant women and its outcome: A community based study. Journal of family medicine and primary care. 2017; 6(4): 739.
13. Viveki RG, Halappanavar AB, Viveki PR, et al. Prevalence of anaemia and its epidemiological determinants in pregnant women. Al Ameen J Med Sci. 2012; 5(3): 216-3.
14. Toteja GS, Singh P, Dhillon BS, et al. Prevalence of anemia among pregnant women and adolescent girls in 16 districts of India. Food and Nutrition Bulletin. 2006; 27(4): 311-5.
15. Gautam VP, Bansal Y, Taneja OK, et al. Prevalence of anaemia amongst pregnant women and its socio-demographic associates in a rural area of Delhi. Indian Journal of Community Medicine. 2002; 27(4): 157.
16. Tiwari J, Linson CC. A Study on Prevalence of Anemia among Pregnant Women Attending Antenatal Clinic at Rural Health Centre (RHC) and Hospital, Jabalpur City, MP. Journal of Pharmaceutical Research International. 2021; 33(49B): 335-42.
17. Lokare PO, Karanjekar VD, Gattani PL, et al. A study of prevalence of anemia and sociodemographic factors associated with anemia among pregnant women in Aurangabad city, India. Annals of Nigerian Medicine. 2012; 6(1): 30.
18. Sahoo S, Panda B. A study of nutritional status of pregnant women of some villages in Balasore district, Orissa. Journal of Human Ecology. 2006; 20(3): 227-32.
19. Siddiqui MZ, Goli S, Reja T, et al. Prevalence of anemia and its determinants among pregnant, lactating, and nonpregnant nonlactating women in India. Sage Open. 2017; 7(3): 2158244017725555.
20. Sarala V, Gopalan U. A study on prevalence of anemia in pregnancy in South India. Int J Reprod Contracept Obstet Gynecol. 2020; 9(1).
21. Ahmad N, Kalakoti P, Bano R, et al. The prevalence of anemia and associated factors in pregnant women in a rural Indian community. AMJ. 2010; 3(5): 276-80.
22. KavithaK,SumayaaS, RavukumarS,et al. A study on nutritional status of pregnant women of rural area in Ramanathapuram district,Tamil Nadu. International Journal of current research. 2011; 3(11).
23. Gautam VP, Taneja DK, Sharma N, et al. Dietary aspects of pregnant women in rural areas of Northern India. Matern Child Nutr. 2008; 4(2): 86-94. doi:10.1111/j.1740-8709.2007.00131.x.
2. World Health Organization. Worldwide prevalence of anaemia 1993-2005: WHO global database on anaemia; 2008.
3. Tolentino K, Friedman JF. An update on anemia in less developed countries. The American journal of tropical medicine and hygiene. 2007; 77(1): 44-51.
4. Balarajan Y, Ramakrishnan U, Özaltin E, et al. Anaemia in low-income and middle-income countries. The lancet. 2011; 378(9809): 2123-35.
5. Crawley J. Reducing the burden of anemia in infants and young children in malaria-endemic countries of Africa: from evidence to action. The Intolerable Burden of Malaria II: What's New, What's Needed: Supplement to Volume 71 (2) of the American Journal of Tropical Medicine and Hygiene. 2004; 71(Suppl): 25-34.
6. Maskey M, Jha N, Poudel SI, et al. Anemia in pregnancy and its associated factors: A study from Eastern Nepal. Nepal journal of epidemiology. 2014; 4(4): 386-92.
7. Abay A, Yalew HW, Tariku A, et al. Determinants of prenatal anemia in Ethiopia. Archives of Public Health. 2017; 75: 1-0.
8. International Institute for Population Sciences (IIPS) and ICF.Assam: NFHS4 (2015-16). [Online]; 2015. Available at: URL: http://rchiips.org/NFHS/NFHS-4Reports/Assam.pdf..
9. Nternational Institute for Population Sciences (IIPS) and ICF. Assam:NFHS3 (2005 -06). [Online]; 2006. Available at: URL: http://rchiips.org/nfhs/pdf/Assam.pdf.
10. International Institute for Population Sciences (IIPS) and ICF.Assam: NFHS5 (2019-20). [Online]; 2020. Available at: URL: https://nhm.assam.gov.in/sites/default/files/swf_utility_folder/departments/nhm_lipl_in_oid_6/ menu/document/factsheet_as.pdf.
11. Saxena V, Srivastava VK, Idris MZ, et al. Nutritional status of rural pregnant women. Indian Journal of community medicine. 2000; 25(3): 104-7.
12. Suryanarayana R, Chandrappa M, Santhuram AN, et al. Prospective study on prevalence of anemia of pregnant women and its outcome: A community based study. Journal of family medicine and primary care. 2017; 6(4): 739.
13. Viveki RG, Halappanavar AB, Viveki PR, et al. Prevalence of anaemia and its epidemiological determinants in pregnant women. Al Ameen J Med Sci. 2012; 5(3): 216-3.
14. Toteja GS, Singh P, Dhillon BS, et al. Prevalence of anemia among pregnant women and adolescent girls in 16 districts of India. Food and Nutrition Bulletin. 2006; 27(4): 311-5.
15. Gautam VP, Bansal Y, Taneja OK, et al. Prevalence of anaemia amongst pregnant women and its socio-demographic associates in a rural area of Delhi. Indian Journal of Community Medicine. 2002; 27(4): 157.
16. Tiwari J, Linson CC. A Study on Prevalence of Anemia among Pregnant Women Attending Antenatal Clinic at Rural Health Centre (RHC) and Hospital, Jabalpur City, MP. Journal of Pharmaceutical Research International. 2021; 33(49B): 335-42.
17. Lokare PO, Karanjekar VD, Gattani PL, et al. A study of prevalence of anemia and sociodemographic factors associated with anemia among pregnant women in Aurangabad city, India. Annals of Nigerian Medicine. 2012; 6(1): 30.
18. Sahoo S, Panda B. A study of nutritional status of pregnant women of some villages in Balasore district, Orissa. Journal of Human Ecology. 2006; 20(3): 227-32.
19. Siddiqui MZ, Goli S, Reja T, et al. Prevalence of anemia and its determinants among pregnant, lactating, and nonpregnant nonlactating women in India. Sage Open. 2017; 7(3): 2158244017725555.
20. Sarala V, Gopalan U. A study on prevalence of anemia in pregnancy in South India. Int J Reprod Contracept Obstet Gynecol. 2020; 9(1).
21. Ahmad N, Kalakoti P, Bano R, et al. The prevalence of anemia and associated factors in pregnant women in a rural Indian community. AMJ. 2010; 3(5): 276-80.
22. KavithaK,SumayaaS, RavukumarS,et al. A study on nutritional status of pregnant women of rural area in Ramanathapuram district,Tamil Nadu. International Journal of current research. 2011; 3(11).
23. Gautam VP, Taneja DK, Sharma N, et al. Dietary aspects of pregnant women in rural areas of Northern India. Matern Child Nutr. 2008; 4(2): 86-94. doi:10.1111/j.1740-8709.2007.00131.x.
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution 4.0 International License. |
