

Volume 13, Issue 1 (1-2024)
JCHR 2024, 13(1): 32-39 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Ghaffari M, Rakhshanderou S, Negarandeh R, Niksadat N, Ramzankhan A, Vasheghani Farahani A. A Protocol for Patient Education Based on Andragogy: A Convergent Parallel Mixed Methods Study. JCHR 2024; 13 (1) :32-39
URL: http://jhr.ssu.ac.ir/article-1-810-en.html
URL: http://jhr.ssu.ac.ir/article-1-810-en.html
Mohtasham Ghaffari1 

 , Sakineh Rakhshanderou1 , Reza Negarandeh2 , Negin Niksadat *3 , Ali Ramzankhan1 , Ali Vasheghani Farahani4
, Sakineh Rakhshanderou1 , Reza Negarandeh2 , Negin Niksadat *3 , Ali Ramzankhan1 , Ali Vasheghani Farahani4
, Sakineh Rakhshanderou1 , Reza Negarandeh2 , Negin Niksadat *3 , Ali Ramzankhan1 , Ali Vasheghani Farahani4
1- Department of Health Education and Promotion, School of Health & safety, Shahid Beheshti University of Medical Sciences. Tehran, Iran
2- Nursing and Midwifery Care Research Center, School of Nursing and Midwifery, Tehran University of Medical Sciences, Tehran, Iran
3- 1. Department of Public Health, Faculty of health, Tehran Medical Sciences, Islamic Azad University, Tehran, Iran 2. Department of Health Education and Promotion, School of Health & safety, Shahid Beheshti University of Medical Sciences. Tehran, Iran ,Neginniksadat@yahoo.com
4- Cardiac primary prevention research center, Cardiovascular Disease Research Institute, Tehran University of Medical Sciences, Tehran, Iran
2- Nursing and Midwifery Care Research Center, School of Nursing and Midwifery, Tehran University of Medical Sciences, Tehran, Iran
3- 1. Department of Public Health, Faculty of health, Tehran Medical Sciences, Islamic Azad University, Tehran, Iran 2. Department of Health Education and Promotion, School of Health & safety, Shahid Beheshti University of Medical Sciences. Tehran, Iran ,
4- Cardiac primary prevention research center, Cardiovascular Disease Research Institute, Tehran University of Medical Sciences, Tehran, Iran
Full-Text [PDF 586 kb]
(2866 Downloads)
| Abstract (HTML) (2002 Views)
1. Department of Health Education and Promotion, School of Health & safety, Shahid Beheshti University of Medical Sciences. Tehran, Iran
2. Nursing and Midwifery Care Research Center, School of Nursing and Midwifery, Tehran University of Medical Sciences, Tehran, Iran
3. Department of Public Health, Faculty of health, Tehran Medical Sciences, Islamic Azad University, Tehran, Iran
4. Cardiac primary prevention research center, Cardiovascular Disease Research Institute, Tehran University of Medical Sciences, Tehran, Iran
How to cite this paper:
Introduction
Methods
Design
Discussion
Conclusion
Acknowledgments
Conflicts of interest
The authors declared no conflict of interest.
Funding
Not applicable.
Ethical considerations
Code of ethics
IR.SBMU.PHNS.REC.1395.34
Authors' contributions
Open access policy
JCHR does not charge readers and their institution for access to its papers. Full text download of all new and archived papers are free of charge.
References
Full-Text: (946 Views)
| A Protocol for Patients' Education Based on Andragogy: A Convergent Parallel Mixed Methods Study |
Mohtasham Ghaffari 1  , Sakineh Rakhshanderou 1 , Reza Negarandeh 2 , Negin Niksadat *3, 1 ,
, Sakineh Rakhshanderou 1 , Reza Negarandeh 2 , Negin Niksadat *3, 1 ,
, Sakineh Rakhshanderou 1 , Reza Negarandeh 2 , Negin Niksadat *3, 1 ,Ali Ramzankhani 1 , Ali Vasheghani Farahani 4
, Ali Vasheghani Farahani 4 1. Department of Health Education and Promotion, School of Health & safety, Shahid Beheshti University of Medical Sciences. Tehran, Iran
2. Nursing and Midwifery Care Research Center, School of Nursing and Midwifery, Tehran University of Medical Sciences, Tehran, Iran
3. Department of Public Health, Faculty of health, Tehran Medical Sciences, Islamic Azad University, Tehran, Iran
4. Cardiac primary prevention research center, Cardiovascular Disease Research Institute, Tehran University of Medical Sciences, Tehran, Iran
| ARTICLE INFO | ABSTRACT | |
| Original Article Received: 19 Dec 2023 Accepted: 15 Apr 2024 |
Background: Patients' education is a key factor in patients' care. The purpose of this study is to design a protocol for a convergent parallel mixed methods study to explore the experiences of patients about their received educations based on andragogy model.
Methods: This convergent parallel mixed method study includes two parallel quantitative and qualitative phases. During the quantitative phase, a cross-sectional survey will be conducted on 350 adult patients who had the history of hospitalization and received patient education from selected hospitals of Tehran, Iran. Sampling method will be random, and data collection tool will be a researcher-made questionnaire based on the principles of andragogy. The questionnaire’s validity and reliability are also measured, and data will be analyzed using SPSS 16. The qualitative phase will be conducted on adult patients who will be recruited purposively with maximum variation from the selected hospitals. Data will be gathered through semi-structured interviews and analyzed by directed content analysis. With regard to mixed method and using aligning convergence method, the results of the two sets of data will be compared or merged to see if the findings confirm or disconfirm each other. In this parallel section, the similarities between quantitative and qualitative results for assessing patient education are discussed and adapted to suit each other based on andragogy.
Conclusions: The findings of this study will provide information regarding defects in patient education, suggesting that the principles of andragogy will develop patient education programs.
Keywords: Patient Education, Mixed Methods Research, Qualitative Research, Andragogy model |
|
Corresponding Author: Negin Niksadat Neginniksadat@yahoo.com |
Ghaffari M, Rakhshanderou S, Negarandeh R, Niksadat N, Ramzankhani A, Vasheghani Farahani A. A Protocol for Patients' Education Based on Andragogy: A Convergent Parallel Mixed Methods Study. J Community Health Research 2024; 13(1): 32-39.
Patient education is an essential aspect of patient care and is considered one of the most important aspects of self-care and health promotion (1). In most industrialized countries, patient education has been recognized as an integral part of disease management programs and it is recommended in European guidelines (2).
According to the findings of meta-analysis, patient education improves self-care behaviors and health-related quality of life and reduces healthcare costs and the recurrence of acute events (3). Patient education is also considered a fundamental component of cardiovascular diseases (CVD) patient care in hospital and community at large (4).
In order to better manage diseases, the education of the patients is important (5).
Redman’s analysis regarding the education of patients over 25 concluded that education is a challenge to health care providers as it best fits exclusive experiences, needs and ideals of a particular patient (6). Moreover, there was a 60% mismatch with Ministry of Health standards concerning hospitals in Iran, Joint Commission accreditation standards for patient education, and family health centers in the United States (5). It has also been reported that less than 50% of patients, have been educated in different fields by healthcare providers and nurses (7).
Healthcare providers face a number of barriers which in turn has a negative impact on patient education. Among these barriers are paternalistic teaching style, lack of counseling skills and ignorance about principles of adult learning and education (8). Andragogy has emerged as one of the dominant frameworks and perhaps the best-known theory of adult learning for the past 40 years (9). Knowles defines it as the “art and science of helping adults to learn” (10).
Knowles’s model of andragogy is based on six assumptions about adult learners:
The need to know: Adult learners need to know why they need to learn. They want to know how learning experience will benefit them.
Self-concept: Adult learners are self-directed/independent learners.
Prior experience: Life-experience serves as a valuable resource, and adults will learn by gleaning from prior knowledge and experiences.
Readiness: Readiness to learn is based on the adult’s perception of what he or she needs to know.
Orientation to learning: Adult learners’ orientation to learning is based on immediate application. It is problem-centered and focuses on current life situations.
Motivation: Adult learners’ motivation to learn is centered on personal gain. Adults are motivated to learn through internal rather than external factors (Figure 1) (1, 10).
According to the findings of meta-analysis, patient education improves self-care behaviors and health-related quality of life and reduces healthcare costs and the recurrence of acute events (3). Patient education is also considered a fundamental component of cardiovascular diseases (CVD) patient care in hospital and community at large (4).
In order to better manage diseases, the education of the patients is important (5).
Redman’s analysis regarding the education of patients over 25 concluded that education is a challenge to health care providers as it best fits exclusive experiences, needs and ideals of a particular patient (6). Moreover, there was a 60% mismatch with Ministry of Health standards concerning hospitals in Iran, Joint Commission accreditation standards for patient education, and family health centers in the United States (5). It has also been reported that less than 50% of patients, have been educated in different fields by healthcare providers and nurses (7).
Healthcare providers face a number of barriers which in turn has a negative impact on patient education. Among these barriers are paternalistic teaching style, lack of counseling skills and ignorance about principles of adult learning and education (8). Andragogy has emerged as one of the dominant frameworks and perhaps the best-known theory of adult learning for the past 40 years (9). Knowles defines it as the “art and science of helping adults to learn” (10).
Knowles’s model of andragogy is based on six assumptions about adult learners:
The need to know: Adult learners need to know why they need to learn. They want to know how learning experience will benefit them.
Self-concept: Adult learners are self-directed/independent learners.
Prior experience: Life-experience serves as a valuable resource, and adults will learn by gleaning from prior knowledge and experiences.
Readiness: Readiness to learn is based on the adult’s perception of what he or she needs to know.
Orientation to learning: Adult learners’ orientation to learning is based on immediate application. It is problem-centered and focuses on current life situations.
Motivation: Adult learners’ motivation to learn is centered on personal gain. Adults are motivated to learn through internal rather than external factors (Figure 1) (1, 10).
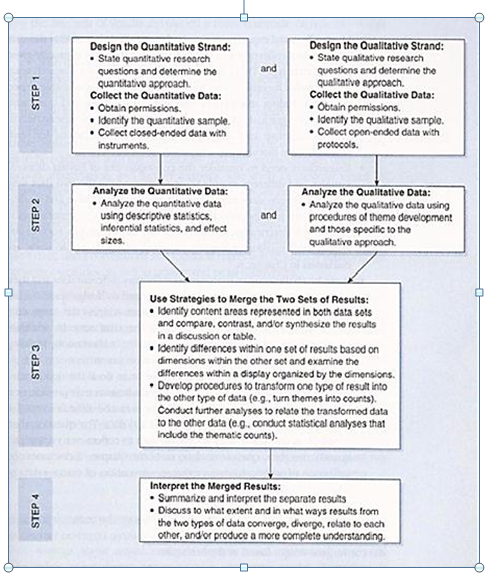
Figure 1. Flowchart of the basic procedures in implementing a convergent design (Creswell et al., 2011) (13)
Studies have shown that educational interventions based on the principles of adult learning with an individualized and patient-centred approach may be a more effective strategy (8, 1, 11). The principles of andragogy can, in fact, be used by healthcare providers, including nurses (1), and it is applicable for all adults who need education on health issues (10).
The application of andragogy to patient education offers healthcare providers a greater understanding of adult patient learning needs and develops teaching tools specific for adult postpartum patient (1). In general, it can be said that the use of theoretical framework in education has been effective to obtain better results (12). Only 20% of studies showed that a theoretical framework guided the educational intervention process. There is little evidence that the principles of andragogy have been effectively utilized to guide education for patients, especially the hospitalized cases (10). In order to improve education and interventions, basic research on present situation is required (1). Understanding deficits in discharge teaching process can also affect nursing education, as more effective patient education practices are introduced (1). Thus, the necessity of this study is based on a number of factors, including: importance and relevance of improving patient education, confirming effectiveness of andragogy in patient education by multiple studies, limited studies on patient education based on andragogy (especially the absence of these studies in a mixed method), and the lack of research in this field in Iran. However, since the topic needs more in-depth information, the use of both quantitative and qualitative data will provide a better understanding of the topic. The aim of this mixed method study is to explore the experiences of patients about their received education based on andragogy model.
Finally, based on the findings, a preventive and cultural-based program or strategy for patient education will be proposed.
Aims
- To explore the experiences of patient education based on the principles of andragogy in a convergent parallel mixed method.
- To assess patient education based on andragogy in terms of patients’ perceptions
- To offer strategies for improving patient education for health care providers.
Finally, based on the findings, a preventive and cultural-based program or strategy for patient education will be proposed.
Aims
- To explore the experiences of patient education based on the principles of andragogy in a convergent parallel mixed method.
- To assess patient education based on andragogy in terms of patients’ perceptions
- To offer strategies for improving patient education for health care providers.
Methods
Design
This study is designed based on convergent parallel mixed methods with quantitative and qualitative phases. In this approach, the researcher collects both quantitative and qualitative data, analyzes them separately, and then compares the results to see if the findings confirm or disconfirm each other (13).
There are four major steps in a convergent design. First, the researcher collects both quantitative and qualitative data about the topic (patient education based on andragogy model). These two types of data collection are concurrent but separate; one does not depend on the results of the other. They also typically have equal importance for addressing the study’s research question. Second, the researcher analyzes the two data sets separately using typical quantitative and qualitative procedures. Once the two sets of initial results are obtained, the researcher reaches the point of interface and works to merge the results of the two data sets in the third step. The merging step may include direct comparison of separate results in the final step. The researcher interprets to what extent and in what ways the two sets of results converge, diverge from each other, relate to each other, and/or combine to create a better understanding in response to the study’s overall purpose (see Figure 2) (13).
Quantitative phase
This phase is a population-based cross-sectional study to assess patient education based on andragogy model in a representative sample of hospitalized adult patients.
There are four major steps in a convergent design. First, the researcher collects both quantitative and qualitative data about the topic (patient education based on andragogy model). These two types of data collection are concurrent but separate; one does not depend on the results of the other. They also typically have equal importance for addressing the study’s research question. Second, the researcher analyzes the two data sets separately using typical quantitative and qualitative procedures. Once the two sets of initial results are obtained, the researcher reaches the point of interface and works to merge the results of the two data sets in the third step. The merging step may include direct comparison of separate results in the final step. The researcher interprets to what extent and in what ways the two sets of results converge, diverge from each other, relate to each other, and/or combine to create a better understanding in response to the study’s overall purpose (see Figure 2) (13).
Quantitative phase
This phase is a population-based cross-sectional study to assess patient education based on andragogy model in a representative sample of hospitalized adult patients.
Sampling
Three hospitals in Tehran will be selected randomly, Shahid Beheshti and Iran University of Medical Sciences. Then, adult patients in the hospitals will be randomly selected as sample. They will be recruited to the study if they are hospitalized, have a history of hospitalization, have the experience of receiving patient education, and agree to share their experiences of patient education. It should be noted that in the sampling process the maximum variation we be considered by taking into account different background variables.
Since there is no information on this issue, to determine the sample size, the authors will consider the maximum value of 0.5 for p and q. Accordingly, 350 adult patients will be required for the study by considering α = 0.05, d = 0.05 and z = 1/96.
Measures
Data will be collected using a research-made questionnaire based on andragogy, which included items regarding demographic information and patients perceptions of patient education based on the 6 principles of andragogy.
Items are guided by the 6 principles of andragogy measuring patients' attitudes and perceptions towards patient education. Questions are rated on a five-point Likert scale.
Development and psychometric evaluation of questionnaire
Psychometric properties of the instrument are determined. The qualitative and quantitative content validity of the items are assessed by an expert review panel (n = 11), and face validity is assessed through patient’s interview (n = 10).
Exploratory and confirmatory factor analyses are performed to test construct validity. The Cranach’s alpha coefficient is done to assess internal consistency of the scale. An alpha value of 0.7 and above is considered acceptable. It is calculated for total scale as 0.95 and each of the 6 domains separately range from 0.72 to 0.94 (the need to know = 0.82, experience = 0.78, self-conception = 0.72, readiness = 0.79, orientation = 0.82 and motivation = 0.92).
Since there is no information on this issue, to determine the sample size, the authors will consider the maximum value of 0.5 for p and q. Accordingly, 350 adult patients will be required for the study by considering α = 0.05, d = 0.05 and z = 1/96.
Measures
Data will be collected using a research-made questionnaire based on andragogy, which included items regarding demographic information and patients perceptions of patient education based on the 6 principles of andragogy.
Items are guided by the 6 principles of andragogy measuring patients' attitudes and perceptions towards patient education. Questions are rated on a five-point Likert scale.
Development and psychometric evaluation of questionnaire
Psychometric properties of the instrument are determined. The qualitative and quantitative content validity of the items are assessed by an expert review panel (n = 11), and face validity is assessed through patient’s interview (n = 10).
Exploratory and confirmatory factor analyses are performed to test construct validity. The Cranach’s alpha coefficient is done to assess internal consistency of the scale. An alpha value of 0.7 and above is considered acceptable. It is calculated for total scale as 0.95 and each of the 6 domains separately range from 0.72 to 0.94 (the need to know = 0.82, experience = 0.78, self-conception = 0.72, readiness = 0.79, orientation = 0.82 and motivation = 0.92).
Data analyses
Descriptive statistics (frequency, mean, and standard deviation) will be used to explore quantitative data. Statistical tests such as independent t-test and Pearson test will be used to estimate correlations at 0.05 level of significance. Data will be analyzed using SPSS 16 statistical software.
Qualitative phase
Sampling
Purposeful sampling strategy will be used. The adult patients in the selected hospitals will be purposively recruited to the study if they are hospitalized, have a history of hospitalization, received patient education, and agree to share their experiences of patient education. Sampling will be done with maximum variation regarding participants’ age, gender, marital status, and educational level.
Data collection
Qualitative data will be collected via semi-structured and in-depth interviews using a pre-established interview guide. The interview guide will consist of open-ended questions based on 6 categories of andragogy model to allow patients to fully explain their own experiences. At the beginning of each interview, the purpose of the study and the individuals’ right to refuse to participate in the study will be explained. Duration of each interview is different based on patient’s situation. Data will be recorded through tape recording and note taking. Data collection will be continued until saturation is reached, and no new themes emerge in the interviews.
Qualitative phase
Sampling
Purposeful sampling strategy will be used. The adult patients in the selected hospitals will be purposively recruited to the study if they are hospitalized, have a history of hospitalization, received patient education, and agree to share their experiences of patient education. Sampling will be done with maximum variation regarding participants’ age, gender, marital status, and educational level.
Data collection
Qualitative data will be collected via semi-structured and in-depth interviews using a pre-established interview guide. The interview guide will consist of open-ended questions based on 6 categories of andragogy model to allow patients to fully explain their own experiences. At the beginning of each interview, the purpose of the study and the individuals’ right to refuse to participate in the study will be explained. Duration of each interview is different based on patient’s situation. Data will be recorded through tape recording and note taking. Data collection will be continued until saturation is reached, and no new themes emerge in the interviews.
Data analyses
Directed content analysis approach will be used. The goal of this method is to conceptually validate or extend a theoretical framework or theory. This research can identify key concepts or variables as initial coding categories. This approach was employed by Hsieh and Shannon in 2005 (14).
Regarding qualitative data analysis, the transcription of interviews will be implemented at the end of each session; the researcher will review it several times in order to achieve a correct understanding. Then, the text will be broken into the smallest meaningful units and codes. Finally, the codes will be classified into six main categories based on andragogy model to reveal the patients’ experience of patient education based on andragogy.
Peer and member check will be performed to assess trustworthiness of data. Moreover, constant comparison method is used during the research. The authors will use MAXQDA10 software to manage qualitative data.
Regarding qualitative data analysis, the transcription of interviews will be implemented at the end of each session; the researcher will review it several times in order to achieve a correct understanding. Then, the text will be broken into the smallest meaningful units and codes. Finally, the codes will be classified into six main categories based on andragogy model to reveal the patients’ experience of patient education based on andragogy.
Peer and member check will be performed to assess trustworthiness of data. Moreover, constant comparison method is used during the research. The authors will use MAXQDA10 software to manage qualitative data.
Data integration
According to the convergent parallel design of this study, the two data sets will be analyzed separately using typical quantitative and qualitative procedures. Then, the two phases will be integrated in order to interpret findings and to see if the findings confirm or disconfirm each other (13). On the other hand, in the mixed part of the convergent type, the results of the two sets of data will be compared or merged to see if the findings confirm or disconfirm each other (13). In this section, the similarities between the quantitative and qualitative results with regard to assessing patient education based on andragogy are discussed and adapted.
According to the findings of this section, strategies based on andragogy model will be developed for the improvement of patient education.
According to the convergent parallel design of this study, the two data sets will be analyzed separately using typical quantitative and qualitative procedures. Then, the two phases will be integrated in order to interpret findings and to see if the findings confirm or disconfirm each other (13). On the other hand, in the mixed part of the convergent type, the results of the two sets of data will be compared or merged to see if the findings confirm or disconfirm each other (13). In this section, the similarities between the quantitative and qualitative results with regard to assessing patient education based on andragogy are discussed and adapted.
According to the findings of this section, strategies based on andragogy model will be developed for the improvement of patient education.
Discussion
Generally, the application of principles of adult learning theory or andragogy in patient education programming was strongly supported by the literature (15-19).
The innovation and strength of this study is that it is the first study on patient education based on andragogy in Iran and the first study with a mixed method design in this case in the world. Moreover, both quantitative and qualitative data are collected and analyzed separately at roughly the same time. Comparing the two types of data will provide a better understanding of the topic. The combination of both quantitative and qualitative methods allows us to understand the patient’s perceptions and experiences regarding patient education. Therefore, defects in patient education can be detected and improved.
Similarly, the findings of a study on CVD patient education indicated that the principles of adult education are not sufficiently observed in CVD adult patient education programs. This study aims to determine the correlation between CVD patient education and the principles of andragogy model only in terms of the quantitative part (20).
Similarly, the findings of a study on CVD patient education indicated that the principles of adult education are not sufficiently observed in CVD adult patient education programs. This study aims to determine the correlation between CVD patient education and the principles of andragogy model only in terms of the quantitative part (20).
Furthermore, the andragogical questionnaire created in this study is the first instrument with sound psychometric qualities to successfully measure andragogical principles in patient education in general. This questionnaire successfully isolates and measures all the andragogy principles, especially in patient education.
To compare this study with other studies, in “Development of a Generalized Instrument to Measure Andragogy” (2009), only five of six andragogical principles were addressed (9).
Similarly, a study in USA (2014) was conducted based on Knowles’ model of andragogy with concurrent parallel mixed-method; the purpose of this study was to gain an understanding on how the structure and process of discharge teaching practices impact successful postpartum teaching. However, the study applied Application of Core Learning Principles to Evidence of Patient-Centered Behavior (EPCBS)) questionnaire to assess the functions of nurses in compliance with the principles of andragogy (1).
Another study on using adult learning principles to improve patient education found that effective education begins with holistic and patient-centered assessment (21). Patient assessment before education can turn education into a more positive experience and enhance patient satisfaction (21, 22, 23, 24).
Similarly, a study in USA (2014) was conducted based on Knowles’ model of andragogy with concurrent parallel mixed-method; the purpose of this study was to gain an understanding on how the structure and process of discharge teaching practices impact successful postpartum teaching. However, the study applied Application of Core Learning Principles to Evidence of Patient-Centered Behavior (EPCBS)) questionnaire to assess the functions of nurses in compliance with the principles of andragogy (1).
Another study on using adult learning principles to improve patient education found that effective education begins with holistic and patient-centered assessment (21). Patient assessment before education can turn education into a more positive experience and enhance patient satisfaction (21, 22, 23, 24).
Conclusion
Hopefully, this study will provide comprehensive basic information about patient education. Problems in the process can affect the patients' education by nurses, doctors, and other healthcare workers. Therefore, they are in better position to educate patients more effectively. The results of this research can be useful in evaluating, measuring, designing, and improving interventions and improving educational programs for nurses, doctors, other staff and care providers in hospitals and health centers.
Acknowledgments
This study was extracted from project No 1396/56489 from the student research committee, Shahid Beheshti University of Medical Sciences, Tehran, Iran. The authors would like to thank the “student research committee” and “Research and Technology chancellor” in Shahid Beheshti University of Medical Sciences for their financial support.
Conflicts of interest
The authors declared no conflict of interest.
Funding
Not applicable.
Ethical considerations
The Ethical Review Committee of Shahid Beheshti University of Medical Sciences approved of this study. The procedures used in this study followed the guidelines of the Declaration of Helsinki. The permission was obtained from authorities in the hospitals, and an informed and verbal consent was taken from the participants who were ensured of the confidentiality of their names and information. They were also informed of their liberty to leave the interview at any phase of the study.
Code of ethics
IR.SBMU.PHNS.REC.1395.34
Authors' contributions
All the authors contributed to the conception and design of the study. NN drafted the first version of the manuscript. NN, MG, SR, and RN revised the manuscript. AV critically reviewed the manuscript for important intellectual content. All the authors approved the final version.
Open access policy
JCHR does not charge readers and their institution for access to its papers. Full text download of all new and archived papers are free of charge.
References
1. Day D. Postpartum patient teaching success: implications from nursing and patient perspectives [PhD Thesis in Education]: Walden University; 2014.
2. Juillière Y, Suty-Selton C, Riant E, et al. Prescription of cardiovascular drugs in the French ODIN cohort of heart failure patients according to age and type of chronic heart failure. Archives of Cardiovascular Diseases. 2014; 107)1(: 21-32.
3. De Melo Ghisi GL, Grace SL, Thomas S, et al. Behavior determinants among cardiac rehabilitation patients receiving educational interventions: An application of the health action process approach. Patient education and counseling. 2015; 98(5): 612-21.
4. Imani A, Imani E. Needs assessment of self-care training in patients with coronary artery disease in Bandar Abbas. Preventive Care in Nursing & Midwifery Journal. 2013; 3(1): 30-37. [Persian]
5. Norouzi H, Tohidi S, Moonaghi HK, et al. The Comporison of the Effects of the Lecture and Self-Learning Module on Nurses, Teaching-Competency to Cardiac Patient Education Cardiac Patient Education. J Mazandaran U Med Sci. 2014; 23(1): 197-202. [Persian]
6. Deyirmenjian M, Karam N, Salameh P. Preoperative patient education for open-heart patients: a source of anxiety? Patient Education and Counseling. 2006; 62(1): 111-117.
7.Tahery N, Razavi Zadegan M, Kaiali M, et al. Importance of Patient education according Abadan nursing students’ opinions. Modern Care Journal. 2011; 8(2): 100-106. [Persian]
8. Boyde M, Grenfell K, Brown R, et al. What have our patients learnt after being hospitalised for an acute myocardial infarction? Australian Critical Care. 2015; 28: 134-139.
9. Holton EF, Wilson LS, Bates RA. Toward development of a generalized instrument to measure andragogy. Human Resource Development Quarterly. 2009; 20(2): 169-93.
10. Knowles MS, Holton EF, Swanson RA. The Adult Learner: The definitive classic in adult education and human resource development Burlington: MA: Elsevier; 2011.
11. Kennedy MBB, Parish AL. Educational theory and cognitive science: Practical principles to improve patient education. Nursing Clinics. 2021; 56(3): 401-12.
12. Hazavehei SMM, Sahabadi S, Hashemi SZ. The role of health education in reducing cardiovascular diseases risk factors: A systematic review. Knowledge and Health. 2014; 9(1): 30-42. [Persian]
13. Creswell JW, Plano Clark VL. Designing and conducting mixed methods research,choosing a mixed methods design, 2nd ed,3rd , SAGE publication;2011.
14. Hsieh HF, Shannon SE. Three approaches to qualitative content analysis. Qual Health Res. 2005; (15): 1277-1288.
15. Templeton HR, Coates VE. Development of an education package for men with prostate cancer on hormonal manipulation therapy. Clinical Effectiveness in Nursing. 2003; 7(1): 33-42.
16. Van Wyk K, Backwell A, Townson A. A narrative literature review to direct spinal cord injury patient education programming. Topics in spinal cord injury rehabilitation. 2015; 21(1): 49-60.
17. Hopstock LA. Motivation and adult learning: A survey among hospital personnel attending a CPR course. Resuscitation. 2008; 76(3): 425-30.
18. Hill CA. Acute heart failure: too sick for discharge teaching? Critical care nursing quarterly. 2009; 32(2): 106-11.
19. Teasdale S, Bainbridge M, editors. Improving information management in family practice: testing an adult learning model. Proceedings of the AMIA Annual Fall Symposium; 1997: American Medical Informatics Association.
20. Niksadat N, Rakhshanderou S, Negarandeh R, Ramezankhani A, Farahani AV, Ghaffari M. Concordance of the cardiovascular patient education with the principles of Andragogy model. Archives of Public Health. 2022; 80(1): 1-10.
21. Kennedy MBB, Parish AL. Educational Theory and Cognitive Science: Practical Principles to Improve Patient Education. Nursing Clinics. 2021; 56(3): 401-12.
22. Mann KS. Education and health promotion for new patients with cancer: A quality improvement model. Clinical journal of oncology nursing. 2011; 15(1): 55.
23. Cullen MW, Geske JB, Anavekar NS, McAdams JA, Beliveau ME, Ommen SR, et al., editors. Reinvigorating continuing medical education: meeting the challenges of the digital age. Mayo Clinic Proceedings; 2019: Elsevier.
24. Sanchez LM, Cooknell LE. The Power of 3: Using adult learning principles to facilitate patient education. Nursing. 2017; 47(2): 17-9.
2. Juillière Y, Suty-Selton C, Riant E, et al. Prescription of cardiovascular drugs in the French ODIN cohort of heart failure patients according to age and type of chronic heart failure. Archives of Cardiovascular Diseases. 2014; 107)1(: 21-32.
3. De Melo Ghisi GL, Grace SL, Thomas S, et al. Behavior determinants among cardiac rehabilitation patients receiving educational interventions: An application of the health action process approach. Patient education and counseling. 2015; 98(5): 612-21.
4. Imani A, Imani E. Needs assessment of self-care training in patients with coronary artery disease in Bandar Abbas. Preventive Care in Nursing & Midwifery Journal. 2013; 3(1): 30-37. [Persian]
5. Norouzi H, Tohidi S, Moonaghi HK, et al. The Comporison of the Effects of the Lecture and Self-Learning Module on Nurses, Teaching-Competency to Cardiac Patient Education Cardiac Patient Education. J Mazandaran U Med Sci. 2014; 23(1): 197-202. [Persian]
6. Deyirmenjian M, Karam N, Salameh P. Preoperative patient education for open-heart patients: a source of anxiety? Patient Education and Counseling. 2006; 62(1): 111-117.
7.Tahery N, Razavi Zadegan M, Kaiali M, et al. Importance of Patient education according Abadan nursing students’ opinions. Modern Care Journal. 2011; 8(2): 100-106. [Persian]
8. Boyde M, Grenfell K, Brown R, et al. What have our patients learnt after being hospitalised for an acute myocardial infarction? Australian Critical Care. 2015; 28: 134-139.
9. Holton EF, Wilson LS, Bates RA. Toward development of a generalized instrument to measure andragogy. Human Resource Development Quarterly. 2009; 20(2): 169-93.
10. Knowles MS, Holton EF, Swanson RA. The Adult Learner: The definitive classic in adult education and human resource development Burlington: MA: Elsevier; 2011.
11. Kennedy MBB, Parish AL. Educational theory and cognitive science: Practical principles to improve patient education. Nursing Clinics. 2021; 56(3): 401-12.
12. Hazavehei SMM, Sahabadi S, Hashemi SZ. The role of health education in reducing cardiovascular diseases risk factors: A systematic review. Knowledge and Health. 2014; 9(1): 30-42. [Persian]
13. Creswell JW, Plano Clark VL. Designing and conducting mixed methods research,choosing a mixed methods design, 2nd ed,3rd , SAGE publication;2011.
14. Hsieh HF, Shannon SE. Three approaches to qualitative content analysis. Qual Health Res. 2005; (15): 1277-1288.
15. Templeton HR, Coates VE. Development of an education package for men with prostate cancer on hormonal manipulation therapy. Clinical Effectiveness in Nursing. 2003; 7(1): 33-42.
16. Van Wyk K, Backwell A, Townson A. A narrative literature review to direct spinal cord injury patient education programming. Topics in spinal cord injury rehabilitation. 2015; 21(1): 49-60.
17. Hopstock LA. Motivation and adult learning: A survey among hospital personnel attending a CPR course. Resuscitation. 2008; 76(3): 425-30.
18. Hill CA. Acute heart failure: too sick for discharge teaching? Critical care nursing quarterly. 2009; 32(2): 106-11.
19. Teasdale S, Bainbridge M, editors. Improving information management in family practice: testing an adult learning model. Proceedings of the AMIA Annual Fall Symposium; 1997: American Medical Informatics Association.
20. Niksadat N, Rakhshanderou S, Negarandeh R, Ramezankhani A, Farahani AV, Ghaffari M. Concordance of the cardiovascular patient education with the principles of Andragogy model. Archives of Public Health. 2022; 80(1): 1-10.
21. Kennedy MBB, Parish AL. Educational Theory and Cognitive Science: Practical Principles to Improve Patient Education. Nursing Clinics. 2021; 56(3): 401-12.
22. Mann KS. Education and health promotion for new patients with cancer: A quality improvement model. Clinical journal of oncology nursing. 2011; 15(1): 55.
23. Cullen MW, Geske JB, Anavekar NS, McAdams JA, Beliveau ME, Ommen SR, et al., editors. Reinvigorating continuing medical education: meeting the challenges of the digital age. Mayo Clinic Proceedings; 2019: Elsevier.
24. Sanchez LM, Cooknell LE. The Power of 3: Using adult learning principles to facilitate patient education. Nursing. 2017; 47(2): 17-9.
Review: Research |
Subject:
Health education
Received: 2023/12/19 | Accepted: 2024/04/15 | Published: 2024/01/21
Received: 2023/12/19 | Accepted: 2024/04/15 | Published: 2024/01/21
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution 4.0 International License. |
