

Volume 14, Issue 1 (1-2025)
JCHR 2025, 14(1): 182-191 |
Back to browse issues page

Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
S S, Dabade K J, Dhadave M, G A. A Study on Prevalence and Pattern of Tobacco Usage among Adults in Manikeshwari, Kalaburagi, Karnataka, India: A Cross-Sectional Study. JCHR 2025; 14 (1) :182-191
URL: http://jhr.ssu.ac.ir/article-1-1129-en.html
URL: http://jhr.ssu.ac.ir/article-1-1129-en.html



1- Department of Community Medicine, Gulbarga Institute of Medical Sciences, Kalaburagi, Karnataka, India , sangitasivarman@gmail.com
2- Department of Community Medicine, Gulbarga Institute of Medical Sciences, Kalaburagi, Karnataka, India
3- Gulbarga Institute of Medical Sciences, Kalaburagi, Karnataka, India
2- Department of Community Medicine, Gulbarga Institute of Medical Sciences, Kalaburagi, Karnataka, India
3- Gulbarga Institute of Medical Sciences, Kalaburagi, Karnataka, India
Full-Text [PDF 644 kb]
(540 Downloads)
| Abstract (HTML) (1037 Views)
How to cite this paper:
Sangita S, Kuldeep Jagannath Dabade, Meenakshi.M Dhadave, Ajaykumar G. A Study on Prevalence and Pattern of Tobacco Usage among Adults in Manikeshwari, Kalaburagi, Karnataka, India: A Cross-Sectional Study. J Community Health Research 2025; 14(1): 182-191.
Introduction
Table 1. Sociodemographic details of participants
Table 2. History of tobacco usage
Table 3. Prevalence and determinants of tobacco usage
Table 4. Pattern of tobacco usage
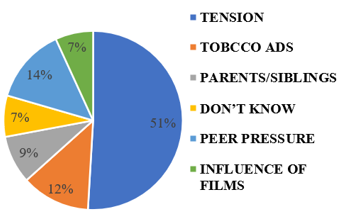
Figure 2 shows that addiction is the main reason for continued tobacco use, cited by 48.9% of participants. Other reasons include lack of existing health issues (15.6%), unwillingness to quit, and gum problems (11.1%). Habit, craving, and other health problems each account for 4.4%. Despite these barriers, only 13.9% of users expressed a willingness to quit in the future, highlighting a significant challenge for cessation efforts.
.PNG)
Table 5. Association between sociodemographic factors and tobacco usage
*Significant at p-value < 0.05
References
Full-Text: (116 Views)
| A Study on Prevalence and Pattern of Tobacco Usage among Adults in Manikeshwari, Kalaburagi, Karnataka, India: A Cross-Sectional Study |

- Department of Community Medicine, Gulbarga Institute of Medical Sciences, Kalaburagi, Karnataka, India
- Gulbarga Institute of Medical Sciences, Kalaburagi, Karnataka, India
| ARTICLE INFO | ABSTRACT | |
| Original Article Received: 17 Feb 2025 Accepted: 16 Jul 2025 |
Background: Tobacco use in India is a significant public health challenge, contributing to high morbidity and mortality. Despite strict regulations, widespread cultural acceptance and accessibility continue to drive its prevalence across diverse population groups. The objective is to estimate prevalence of tobacco, its usage patterns, and their socio-demographic associations among adults in Manikeshwari, Kalaburagi.” Methods: A cross-sectional study was conducted for 2 months among adults residing in Manikeshwari using a pre-tested questionnaire administered through face-to-face interviews. The sample size of 350 was calculated based on a 33.5% prevalence in Kalaburagi, with participants selected through cluster sampling. Data from 310 participants were analyzed for completeness using Jamovi software. Results: Among 310 participants, 41.9% had used tobacco at least once, with 29.7% currently using it. Most smokers (54.9%) commenced between 20 and 30, whereas 23.6% started earlier. 47.6% of users had been consuming tobacco for less than 10 years. Smokeless tobacco was utilized by 63% of the participants. With addiction as the main hurdle (48.9%), only 13.9% of current users are willing to quit. Smoking was found to be associated with gender (p-value: <0.001), religion (p-value: 0.02), marital status(p-value:<0.03), education(p-value:<0.001), and occupation(p-value:<0.001). Conclusion: The study shows high tobacco use, mainly smokeless forms, starting in early adulthood, influenced by demographic and socio-cultural factors. Targeted interventions and stricter enforcement of sales bans and no-tobacco zone regulations are recommended. Keywords: Epidemiology, Tobacco Use Disorder, Adults, Urban population |
|
 |
||
Corresponding Author: Sangita S sangitasivaraman@gmail.com |
Sangita S, Kuldeep Jagannath Dabade, Meenakshi.M Dhadave, Ajaykumar G. A Study on Prevalence and Pattern of Tobacco Usage among Adults in Manikeshwari, Kalaburagi, Karnataka, India: A Cross-Sectional Study. J Community Health Research 2025; 14(1): 182-191.
Introduction
Tobacco use is a leading global cause of preventable morbidity and mortality, with the majority of users starting during adolescence and establishing long-term habits by their late twenties. The Southeast Asian Region had the highest prevalence of tobacco use globally in 2020, with India contributing significantly to this burden. According to the Global Adult Tobacco Survey (GATS-2), 28.6% of Indian adults aged 15 and above, approximately 266.8 million people, currently use tobacco products (1,2). Tobacco imposes a heavy health and economic burden, consuming about 5% of India’s health spending in 2017–18, with smoking responsible for 74% of these costs and men contributing to 91% of the economic impact (3).
Despite the existence of tobacco control measures such as the Cigarettes and Other Tobacco Products Act (COTPA), taxation, bans on advertising, and public smoking restrictions, tobacco continues to be widely used in India. Its affordability, accessibility, and persistent myths regarding its benefits contribute to its continued prevalence (4,5). In addition to active tobacco use, second-hand smoke exposure remains a significant concern, with four in ten Indian households reporting at least one tobacco user (6).
Tobacco is consumed in both smoked and smokeless forms in India, with beedis (48%) and chewing tobacco (38%) being more commonly used, compared with cigarettes (14%) (2). These patterns vary significantly across regions, socioeconomic strata, and cultural backgrounds. Importantly, tobacco consumption is linked to approximately 56.4% of cancer cases in men and 44.9% cases in women in India (7). The country ranks second globally in total tobacco consumption, after China, with regional disparities in prevalence. In Karnataka, 27.1% of men and 8.5% of women use tobacco, while in Kalaburagi district, the prevalence is even higher, 33.5% among men and 11% among women (8).
Most studies have focused on national and urban populations, leaving rural and semi-urban areas underrepresented. The lack of region-specific data hinders targeted interventions tailored to local needs. Semi-urban districts like Kalaburagi, where tobacco use remains high despite national control measures, are particularly neglected. There is limited knowledge about how sociodemographic factors — including age, education, occupation, income, and caste — influence tobacco use in these settings. Research rarely addresses local enforcement of tobacco laws or the community’s knowledge, attitudes, and practices around tobacco consumption. Early initiation of tobacco use is linked to higher dependence and lower quit rates, underscoring the need for locally focused data (9). This study aims to estimate the prevalence and patterns of tobacco use in Kalaburagi and examine their association with sociodemographic factors, providing essential evidence to inform effective, localized public health strategies.
Methods
A cross-sectional study was conducted among residents of Manikeshwari Kalaburagi who aged >19 for a period of two months in 2024. Based on the prevalence of tobacco usage in Kalaburagi, which was found to be 33.5%, the sample size was calculated with a 95% confidence level and 5% permissible error by using the formula, n = z² pq/ d² (9). The sample size was found to be 342, which was approximated to 350. The participants were chosen through two-stage cluster sampling. In the first stage, Manikeshwari, having a population of 46290, was divided into 4 wards. During the second stage of sampling, to get a sample of 350, 88 people were chosen from each ward through systematic random sampling by selecting every 5th house. The individuals who were 19 and above, and residents of Manikeshwari for at least two years who were willing to participate in the study were included. This was while people who were deaf, dumb, had psychiatric problems, denied consent, and entered incomplete data were excluded from the study. Verbal consent was obtained from participants before the initiation of study.
Data collection method
A door-to-door survey was conducted in the urban field practice area of Gulbarga Institute of Medical Sciences (GIMS) in Manikeshwari, Kalaburagi, and participants were included based on inclusion criteria. The study was explained to them and verbal consent was obtained. The participants were interviewed using a pre-designed, pre-tested, and semi-structured questionnaire (7,10,11). It consisted of two sections: sociodemographic profile and pattern of usage of tobacco products. Participants were categorized as per the operational definitions provided by WHO (12).
Statistical methods
Data were entered in a Microsoft Excel spreadsheet and analyzed using Jamovi software 2.4.14. Results were analyzed with frequency and proportion. The chi-square test was used to find out the association between socio-demographic profile and tobacco usage.
Results
Table 1 presents a detailed overview of the participants’ sociodemographic characteristics. Over half of the individuals (55.4%) aged between 20 and 40, with males comprising a significant majority at 76.2%. 51.6% completed either secondary or higher secondary schooling, while 36.5% comprised skilled and semi-skilled workers. Marital status shows that most participants (76.8%) were married, wherein 66.1% lived in a nuclear family compared to joint families (23.5%) and three-generation families (10.3%). Based on the modified BG Prasad classification, a substantial portion fell within the middle (35.8%) and lower-middle (31.6%) socioeconomic class, while only a small fraction (6.5%) belonged to the upper class.
Despite the existence of tobacco control measures such as the Cigarettes and Other Tobacco Products Act (COTPA), taxation, bans on advertising, and public smoking restrictions, tobacco continues to be widely used in India. Its affordability, accessibility, and persistent myths regarding its benefits contribute to its continued prevalence (4,5). In addition to active tobacco use, second-hand smoke exposure remains a significant concern, with four in ten Indian households reporting at least one tobacco user (6).
Tobacco is consumed in both smoked and smokeless forms in India, with beedis (48%) and chewing tobacco (38%) being more commonly used, compared with cigarettes (14%) (2). These patterns vary significantly across regions, socioeconomic strata, and cultural backgrounds. Importantly, tobacco consumption is linked to approximately 56.4% of cancer cases in men and 44.9% cases in women in India (7). The country ranks second globally in total tobacco consumption, after China, with regional disparities in prevalence. In Karnataka, 27.1% of men and 8.5% of women use tobacco, while in Kalaburagi district, the prevalence is even higher, 33.5% among men and 11% among women (8).
Most studies have focused on national and urban populations, leaving rural and semi-urban areas underrepresented. The lack of region-specific data hinders targeted interventions tailored to local needs. Semi-urban districts like Kalaburagi, where tobacco use remains high despite national control measures, are particularly neglected. There is limited knowledge about how sociodemographic factors — including age, education, occupation, income, and caste — influence tobacco use in these settings. Research rarely addresses local enforcement of tobacco laws or the community’s knowledge, attitudes, and practices around tobacco consumption. Early initiation of tobacco use is linked to higher dependence and lower quit rates, underscoring the need for locally focused data (9). This study aims to estimate the prevalence and patterns of tobacco use in Kalaburagi and examine their association with sociodemographic factors, providing essential evidence to inform effective, localized public health strategies.
Methods
A cross-sectional study was conducted among residents of Manikeshwari Kalaburagi who aged >19 for a period of two months in 2024. Based on the prevalence of tobacco usage in Kalaburagi, which was found to be 33.5%, the sample size was calculated with a 95% confidence level and 5% permissible error by using the formula, n = z² pq/ d² (9). The sample size was found to be 342, which was approximated to 350. The participants were chosen through two-stage cluster sampling. In the first stage, Manikeshwari, having a population of 46290, was divided into 4 wards. During the second stage of sampling, to get a sample of 350, 88 people were chosen from each ward through systematic random sampling by selecting every 5th house. The individuals who were 19 and above, and residents of Manikeshwari for at least two years who were willing to participate in the study were included. This was while people who were deaf, dumb, had psychiatric problems, denied consent, and entered incomplete data were excluded from the study. Verbal consent was obtained from participants before the initiation of study.
Data collection method
A door-to-door survey was conducted in the urban field practice area of Gulbarga Institute of Medical Sciences (GIMS) in Manikeshwari, Kalaburagi, and participants were included based on inclusion criteria. The study was explained to them and verbal consent was obtained. The participants were interviewed using a pre-designed, pre-tested, and semi-structured questionnaire (7,10,11). It consisted of two sections: sociodemographic profile and pattern of usage of tobacco products. Participants were categorized as per the operational definitions provided by WHO (12).
Statistical methods
Data were entered in a Microsoft Excel spreadsheet and analyzed using Jamovi software 2.4.14. Results were analyzed with frequency and proportion. The chi-square test was used to find out the association between socio-demographic profile and tobacco usage.
Results
Table 1 presents a detailed overview of the participants’ sociodemographic characteristics. Over half of the individuals (55.4%) aged between 20 and 40, with males comprising a significant majority at 76.2%. 51.6% completed either secondary or higher secondary schooling, while 36.5% comprised skilled and semi-skilled workers. Marital status shows that most participants (76.8%) were married, wherein 66.1% lived in a nuclear family compared to joint families (23.5%) and three-generation families (10.3%). Based on the modified BG Prasad classification, a substantial portion fell within the middle (35.8%) and lower-middle (31.6%) socioeconomic class, while only a small fraction (6.5%) belonged to the upper class.
Table 1. Sociodemographic details of participants
| Socio-demographic profile |
Category | Frequency (N = 310) |
Percentage (%) |
| Age (in years) | 20-30 | 80 | 25.8 |
| 30-40 | 92 | 29.7 | |
| 40-50 | 63 | 20.3 | |
| 50-60 | 39 | 12.6 | |
| > 60 | 36 | 11.6 | |
| Gender | Male | 237 | 76.5 |
| Female | 73 | 23.5 | |
Education |
Illiterate | 63 | 20.3 |
| Primary | 38 | 12.3 | |
| Secondary and higher secondary | 160 | 51.6 | |
| Graduate and above | 49 | 15.8 | |
| Occupation | Professional | 30 | 9.7 |
| Semi Professional | 31 | 10.0 | |
| Skilled/ semi- skilled | 113 | 36.5 | |
| Unskilled | 49 | 15.7 | |
| Unemployed | 87 | 28.1 | |
| Marital status | Married | 238 | 76.8 |
| Unmarried | 58 | 18.7 | |
| Widowed/separated | 14 | 4.5 | |
| Family type | Nuclear | 205 | 66.2 |
| Joint family | 73 | 23.5 | |
| Three generation family | 32 | 10.3 | |
| Religion | Hindu | 296 | 95.5 |
| Muslim | 14 | 4.5 | |
| Caste | General | 78 | 25.2 |
| OBC | 29 | 9.4 | |
| SC/ST | 203 | 65.4 | |
| Socio-economic class (according to modified B.G. Prasad classification) |
Upper class | 20 | 6.5 |
| Upper middle class | 57 | 18.4 | |
| Middle class | 111 | 35.8 | |
| Lower middle class | 98 | 31.6 | |
| Lower class | 24 | 7.7 |
Table 2 summarizes tobacco use history among participants. Around 41.9% have used tobacco at some point, and most users (54.9%) began at an early age (20–30). Nearly half (47.6%) used tobacco for under 10 years, 34.6% for 10–20 years, and a few reported longer usages. The influence of family and social circles on tobacco use is evident, as 42.3% of participants reported having family or friends who use tobacco. Smokeless tobacco is the most prevalent (65.3%), followed by smoking forms (23.8%) and dual use (10.7%).
Table 2. History of tobacco usage
| History | Categories | Frequency (N = 310) |
Percentage (%) |
| Have you used tobacco at any time in your life? |
Yes | 130 | 41.9 |
| No | 180 | 58.1 | |
| Does anyone in your family or friends use tobacco? |
Yes | 131 | 42.3 |
| No | 179 | 57.7 | |
| Categories | Frequency (N = 130) |
Percentage (%) |
|
| Age of onset of tobacco usage (in years) (N=130) |
10-20 | 31 | 23.8 |
| 20-30 | 72 | 55.4 | |
| 30-40 | 20 | 15.4 | |
| > 40 | 7 | 5.4 | |
| Duration of use (in years) | < 10 | 62 | 47.7 |
| 10-20 | 45 | 34.6 | |
| 20-30 | 15 | 11.5 | |
| ≥ 30 | 8 | 6.2 | |
| Type of tobacco used | Smoking | 31 | 23.9 |
| Smokeless | 85 | 65.3 | |
| Mixed type | 14 | 10.8 |
Table 3 shows the prevalence and determinants of tobacco usage based on age, gender, and type of tobacco. The data revealed that 29.7% of the participants are current tobacco users, with the highest prevalence (33.6%) among young adults within 20–30 age group. There is a significant gender disparity in tobacco use, with males comprising 94.5% of current users, while females account for only 5.4%. Regarding the type of tobacco used, smokeless tobacco is the predominant choice (63%), followed by smoking (23.9%) and mixed-use (13.1%). Most users-initiated tobacco use between the ages of 20–30 (55.4%), while 23.8% began as early as 10–20. In terms of duration, nearly half (47.7%) have been using tobacco for less than 10 years. These findings highlight early initiation, male predominance, and a strong preference for smokeless tobacco.
Table 3. Prevalence and determinants of tobacco usage
| Variables | Category | Number (n = 92) |
Percentage (%) |
| Do you currently use tobacco? | Yes | 92 | 29.7 |
| No | 218 | 70.3 | |
| Age (In Years) | 20-30 | 31 | 33.7 |
| 30-40 | 26 | 28.3 | |
| 40-50 | 15 | 16.3 | |
| 50-60 | 14 | 15.2 | |
| > 60 | 6 | 6.5 | |
| Gender | Male | 87 | 94.6 |
| Female | 5 | 5.4 | |
| Type of Tobacco Usage | Smoking | 22 | 23.9 |
| Smokeless | 58 | 63.0 | |
| Mixed Use | 12 | 13.1 |
Table 4 represents the pattern of tobacco usage among the participants. The pattern of tobacco usage in terms of packet consumption shows that nearly half of users (48.6%) consume 1-5 packets per day, while a substantial portion (35.7%) consumes 5-10 packets daily. A smaller group consumes >10 packets per day (15.7%). For cigarette smokers, the majority (81.6%) are light smokers while 18.3% are moderate smokers.
Table 4. Pattern of tobacco usage
| Tobacco products | Categories | Frequency (N = 70) |
Percentage (%) |
| Number of packets per day | 1-5 | 34 | 48.6 |
| 5-10 | 25 | 35.7 | |
| > 10 | 11 | 15.7 | |
| Quantity/day | (N = 34) | (%) | |
| Number of cigarettes per day | Light smokers | 22 | 64.7 |
| Moderate smokers | 12 | 35.3 |
Figure 1 illustrates the reasons for initiating tobacco use among participants. The most common reason is "tension," reported by over half (51%) of the respondents. This is followed by "peer pressure" (14%) and "tobacco ads" (12%).
Figure 1. Reasons for initiation of tobacco
Figure 2 shows that addiction is the main reason for continued tobacco use, cited by 48.9% of participants. Other reasons include lack of existing health issues (15.6%), unwillingness to quit, and gum problems (11.1%). Habit, craving, and other health problems each account for 4.4%. Despite these barriers, only 13.9% of users expressed a willingness to quit in the future, highlighting a significant challenge for cessation efforts.
Figure 2. Reasons for not quitting tobacco
Table 5 lists the association between various sociodemographic factors and tobacco usage among study participants. The statistically significant risk factors for tobacco usage were gender (p-value < 0.001), religion (p-value = 0.02), education (p-value < 0.001), occupation (p-value < 0.001), and marital status (p-value = 0.03), while the other risk factors were insignificant.
Table 5. Association between sociodemographic factors and tobacco usage
| Sociodemographic factors | Number (N=310) |
Percentage (%) |
Tobacco Yes |
Tobacco No |
P-value | |||
| (N=130) | (%) | (N=180) | (%) | |||||
| Age (in years) |
20-30 | 80 | 25.8 | 36 | 45.0 | 44 | 55.0 | 0.21 |
| 30-40 | 92 | 29.7 | 36 | 39.1 | 56 | 60.9 | ||
| 40-50 | 63 | 20.3 | 27 | 42.9 | 36 | 57.1 | ||
| 50-60 | 39 | 12.6 | 21 | 53.8 | 18 | 46.2 | ||
| ≥60 | 36 | 11.6 | 10 | 27.8 | 26 | 72.2 | ||
| Gender | Male | 237 | 76.5 | 120 | 50.6 | 117 | 49.4 | <0.001* |
| Female | 73 | 23.5 | 10 | 13.7 | 63 | 86.3 | ||
| Religion | Hindu | 296 | 95.5 | 120 | 40.5 | 176 | 59.5 | 0.02* |
| Muslim | 14 | 4.5 | 10 | 71.4 | 4 | 28.6 | ||
| Caste | General | 78 | 25.2 | 36 | 46.2 | 42 | 53.8 | 0.53 |
| OBC | 29 | 9.4 | 10 | 34.5 | 19 | 65.5 | ||
| SC/ST | 203203 203 |
65.4 | 84 | 41.4 | 119 | 58.6 | ||
| Education | Illiterate | 63 | 20.3 | 49 | 77.8 | 14 | 22.2 | < 0.001* |
| Primary | 38 | 12.3 | 22 | 57.9 | 16 | 42.1 | ||
| Secondary | 80 | 25.8 | 40 | 50.0 | 40 | 50.0 | ||
| Higher secondary | 80 | 25.8 | 24 | 30.0 | 56 | 70.0 | ||
| Graduate and above | 49 | 15.8 | 20 | 40.8 | 29 | 59.2 | ||
| Occupation | Professional | 30 | 9.7 | 9 | 30.0 | 21 | 70.0 | < 0.001* |
| Semi professional | 31 | 10.0 | 15 | 48.9 | 16 | 51.6 | ||
| Skilled/ Semi skilled | 105 | 33.9 | 56 | 53.3 | 49 | 46.7 | ||
| Unskilled | 57 | 18.3 | 27 | 47.4 | 30 | 52.6 | ||
| Unemployed | 87 | 28.1 | 23 | 26.4 | 64 | 73.6 | ||
| Marital status | Married | 238 | 76.8 | 90 | 37.8 | 148 | 62.1 | 0.03* |
| Unmarried | 58 | 18.7 | 33 | 51.7 | 25 | 43.1 | ||
| Widowed/ separated | 14 | 4.5 | 7 | 50.0 | 7 | 50.0 | ||
| Family type | Nuclear | 205 | 66.1 | 88 | 42.9 | 117 | 57.1 | 0.66 |
| Joint family | 73 | 23.5 | 31 | 42.5 | 42 | 57.5 | ||
| Three generation family | 32 | 10.4 | 11 | 34.4 | 21 | 65.7 | ||
| Socio-economic class | Upper class | 20 | 6.5 | 3 | 15.0 | 17 | 85.0 | 0.12 |
| Upper middle class | 57 | 18.4 | 22 | 38.6 | 35 | 61.4 | ||
| Middle class | 111 | 35.8 | 51 | 45.9 | 60 | 54.1 | ||
| Lower middle class | 98 | 31.6 | 43 | 43.9 | 55 | 56.1 | ||
| Lower class | 24 | 7.7 | 11 | 45.8 | 13 | 54.2 | ||
Discussion
This study aimed to examine key aspects of tobacco use within the community. Among the 310 participants, the largest proportion (29.6%) were aged 30–40, aligning with the findings by Kulkarni et al., who reported a similar distribution (34.5%) (7). Regarding education, 51.6% of participants had completed secondary or higher secondary education, which was higher than the 44.95% reported by Vansh Maheshwari et al (13).
The prevalence of tobacco use in this study was 29.7%, consistent with findings from similar studies (3, 10). The age of initiation was predominantly between 21–30 (68.8%), followed by 10–20 (18.8%), reflecting patterns similar to those reported by Kulkarni RR et al. (7). These findings suggest that young adults are particularly susceptible to social influences, peer pressure, and gaps in the enforcement of age restrictions. Tobacco use was more prevalent among males (36.7%), a finding corroborated by other studies (3,7,10). This could be attributed to greater social acceptance of tobacco use among men, as well as gender-related differences in risk-taking behavior. The study also noted higher tobacco use among individuals with lower educational attainment, consistent with the findings by Rani M et al. (14), indicating limited awareness about the health risks of tobacco and reduced access to cessation resources. While Sukumar M et al. reported higher tobacco use among married individuals, the present study found a higher prevalence among unmarried and widowed individuals, suggesting that marital responsibilities may deter usage (15).
Furthermore, 63% of participants used smokeless tobacco, a significantly higher proportion compared to the 21.3% reported by Anusha Viswanathan et al., likely reflecting regional and cultural differences where smokeless forms of tobacco are more accessible and socially accepted (16).
Stress emerged as the leading reason for initiating tobacco use, aligning with the findings of Nichter M et al. (17). Advertising also played a significant role, highlighting the impact of aggressive marketing tactics targeting youth through social media and celebrity endorsements. Addiction was identified as the main barrier to quitting, consistent with studies by Shridevi et al. and Gupta R et al., which emphasized the role of long-term dependence and low self-efficacy in sustaining tobacco use (18, 19). Willingness to quit was noted in only 13.9% of the participants, significantly lower than the 76% reported by Kulkarni et al. and the 74.6% reported by Chockalingam et al., indicating lower motivation to quit in this population (7, 20).
Factors such as age, gender, religion, caste, marital status, education, and occupation were associated with tobacco use, in line with findings by Benojir Ahammed et al (21). Recognizing these associations is vital for public health policy, as it enables the National Tobacco Control Programme (NTCP) and supports India’s commitments under the WHO Framework Convention on Tobacco Control (WHO-FCTC) to implement targeted, culturally sensitive interventions and behavior change communication strategies aimed at high-risk groups.
Strengths and limitations of the study
The study captures comprehensive patterns of tobacco use, including both smoking and smokeless forms, in a specific urban population. Its inclusion of key sociodemographic factors and use of a validated tool strengthens the relevance and reliability of the findings. The study's cross-sectional design limits causal inference and the ability to track changes over time. Self-reported data may be influenced by recall or social desirability bias. Generalizability is limited.
Conclusion
The study provides comprehensive insights into the prevalence, patterns, and awareness of tobacco use among adults in Manikeshwari, Kalaburagi. A substantial proportion of participants reported current or past tobacco use, with smokeless tobacco being the most commonly used form. Initiation was most frequent during early adulthood, highlighting a critical window for preventive efforts. Health concerns and family influence were major motivators for quitting, while addiction emerged as the primary barrier. These findings emphasize the need for targeted public health interventions under programs like NTCP, focusing on early education, broader health risk communication, and addiction-centered cessation support, particularly for smokeless tobacco users.
Recommendations and future scope
In light of the study’s findings, there is a pressing need for targeted public health strategies to curb tobacco use in Manikeshwari, Kalaburagi. Educational campaigns should focus on raising awareness about the dangers of both smoking and smokeless tobacco, particularly among adolescents and individuals with limited literacy. Preventive measures such as school-based interventions, strict enforcement of age-related sales restrictions, and penalties in designated tobacco-free areas are essential to discourage early initiation. Enhancing cessation efforts through accessible support systems, community participation, and encouragement from family members is equally important. Future studies should consider longitudinal research to monitor evolving usage trends and evaluate the effectiveness of existing interventions. Exploring underlying psychosocial and socioeconomic influences, such as stress, peer dynamics, education, and income, can aid in developing more tailored prevention programs. Additionally, research focusing on youth, gender-based differences, local policy impact, and program evaluations will offer valuable insights. Cross-regional comparisons may also uncover localized drivers of tobacco use, enabling the development of more effective, region-specific control measures.
Acknowledgement
The authors would like to thank all authors and participants for their immense support.
Conflicts of interest
The authors declared no conflicts of interest.
Funding
No funding was received for conducting this study.
Data availability
All data generated or analyzed during this study are included in this published article.
Ethical considerations
Institutional Ethics Committee of Gulbarga Institute of Medical Sciences, Kalaburagi approved the study.
Code of ethical
The manuscript was prepared according to STROBE guidelines.
Authors contribution
S. S and K. J. D did data collection, review of literature, methodology, data analysis and interpretation, writing-original draft and editing; M. M.D and A. G were involved in conceptualization, supervision, writing-review.
Open access policy
JCHR does not charge readers and their institutions for access to its papers. Full text downloads of all new and archived papers are free of charge.
Abbreviations
SEAR Southeast Asian Region
OBC Other Backward Class
WHO World Health Organization
SC/ST Scheduled Castes/Scheduled Tribes
GATS Global Adult Tobacco Survey
GIMS Gulbarga Institute of Medical Sciences
COTPA Act Cigarettes and Other Tobacco Products Act
This study aimed to examine key aspects of tobacco use within the community. Among the 310 participants, the largest proportion (29.6%) were aged 30–40, aligning with the findings by Kulkarni et al., who reported a similar distribution (34.5%) (7). Regarding education, 51.6% of participants had completed secondary or higher secondary education, which was higher than the 44.95% reported by Vansh Maheshwari et al (13).
The prevalence of tobacco use in this study was 29.7%, consistent with findings from similar studies (3, 10). The age of initiation was predominantly between 21–30 (68.8%), followed by 10–20 (18.8%), reflecting patterns similar to those reported by Kulkarni RR et al. (7). These findings suggest that young adults are particularly susceptible to social influences, peer pressure, and gaps in the enforcement of age restrictions. Tobacco use was more prevalent among males (36.7%), a finding corroborated by other studies (3,7,10). This could be attributed to greater social acceptance of tobacco use among men, as well as gender-related differences in risk-taking behavior. The study also noted higher tobacco use among individuals with lower educational attainment, consistent with the findings by Rani M et al. (14), indicating limited awareness about the health risks of tobacco and reduced access to cessation resources. While Sukumar M et al. reported higher tobacco use among married individuals, the present study found a higher prevalence among unmarried and widowed individuals, suggesting that marital responsibilities may deter usage (15).
Furthermore, 63% of participants used smokeless tobacco, a significantly higher proportion compared to the 21.3% reported by Anusha Viswanathan et al., likely reflecting regional and cultural differences where smokeless forms of tobacco are more accessible and socially accepted (16).
Stress emerged as the leading reason for initiating tobacco use, aligning with the findings of Nichter M et al. (17). Advertising also played a significant role, highlighting the impact of aggressive marketing tactics targeting youth through social media and celebrity endorsements. Addiction was identified as the main barrier to quitting, consistent with studies by Shridevi et al. and Gupta R et al., which emphasized the role of long-term dependence and low self-efficacy in sustaining tobacco use (18, 19). Willingness to quit was noted in only 13.9% of the participants, significantly lower than the 76% reported by Kulkarni et al. and the 74.6% reported by Chockalingam et al., indicating lower motivation to quit in this population (7, 20).
Factors such as age, gender, religion, caste, marital status, education, and occupation were associated with tobacco use, in line with findings by Benojir Ahammed et al (21). Recognizing these associations is vital for public health policy, as it enables the National Tobacco Control Programme (NTCP) and supports India’s commitments under the WHO Framework Convention on Tobacco Control (WHO-FCTC) to implement targeted, culturally sensitive interventions and behavior change communication strategies aimed at high-risk groups.
Strengths and limitations of the study
The study captures comprehensive patterns of tobacco use, including both smoking and smokeless forms, in a specific urban population. Its inclusion of key sociodemographic factors and use of a validated tool strengthens the relevance and reliability of the findings. The study's cross-sectional design limits causal inference and the ability to track changes over time. Self-reported data may be influenced by recall or social desirability bias. Generalizability is limited.
Conclusion
The study provides comprehensive insights into the prevalence, patterns, and awareness of tobacco use among adults in Manikeshwari, Kalaburagi. A substantial proportion of participants reported current or past tobacco use, with smokeless tobacco being the most commonly used form. Initiation was most frequent during early adulthood, highlighting a critical window for preventive efforts. Health concerns and family influence were major motivators for quitting, while addiction emerged as the primary barrier. These findings emphasize the need for targeted public health interventions under programs like NTCP, focusing on early education, broader health risk communication, and addiction-centered cessation support, particularly for smokeless tobacco users.
Recommendations and future scope
In light of the study’s findings, there is a pressing need for targeted public health strategies to curb tobacco use in Manikeshwari, Kalaburagi. Educational campaigns should focus on raising awareness about the dangers of both smoking and smokeless tobacco, particularly among adolescents and individuals with limited literacy. Preventive measures such as school-based interventions, strict enforcement of age-related sales restrictions, and penalties in designated tobacco-free areas are essential to discourage early initiation. Enhancing cessation efforts through accessible support systems, community participation, and encouragement from family members is equally important. Future studies should consider longitudinal research to monitor evolving usage trends and evaluate the effectiveness of existing interventions. Exploring underlying psychosocial and socioeconomic influences, such as stress, peer dynamics, education, and income, can aid in developing more tailored prevention programs. Additionally, research focusing on youth, gender-based differences, local policy impact, and program evaluations will offer valuable insights. Cross-regional comparisons may also uncover localized drivers of tobacco use, enabling the development of more effective, region-specific control measures.
Acknowledgement
The authors would like to thank all authors and participants for their immense support.
Conflicts of interest
The authors declared no conflicts of interest.
Funding
No funding was received for conducting this study.
Data availability
All data generated or analyzed during this study are included in this published article.
Ethical considerations
Institutional Ethics Committee of Gulbarga Institute of Medical Sciences, Kalaburagi approved the study.
Code of ethical
The manuscript was prepared according to STROBE guidelines.
Authors contribution
S. S and K. J. D did data collection, review of literature, methodology, data analysis and interpretation, writing-original draft and editing; M. M.D and A. G were involved in conceptualization, supervision, writing-review.
Open access policy
JCHR does not charge readers and their institutions for access to its papers. Full text downloads of all new and archived papers are free of charge.
Abbreviations
SEAR Southeast Asian Region
OBC Other Backward Class
WHO World Health Organization
SC/ST Scheduled Castes/Scheduled Tribes
GATS Global Adult Tobacco Survey
GIMS Gulbarga Institute of Medical Sciences
COTPA Act Cigarettes and Other Tobacco Products Act
References
- Gupta A, Grover S, Sakrawal K, et al. Prevalence, Patterns, and Predictors of Tobacco Consumption among Adolescents: An Observational Study from a Rural area of Rajasthan. Indian Journal of Community Medicine. 2023; 48(5): 748-54.
- Pahari S, Barman D, Talukdar R. Tobacco usage in India: A meta‐analysis of evidence drawn from regional studies between 2010 and 2022. Tropical Medicine & International Health. 2023; 28(9): 699-709.
- Chawla A. The worrying patterns of tobacco consumption in India. Centre for Economic Data and Analysis (CEDA), Ashoka University; 2022. Available at: URL: ceda.ashoka.edu.in
- Shah S, Dave B, Shah R, et al. Socioeconomic and cultural impact of tobacco in India. Journal of family medicine and primary care. 2018; 7(6): 1173-6.
- Hosseinpoor AR, Parker LA, Tursan d'Espaignet E, et al. Social determinants of smoking in low-and middle-income countries: results from the World Health Survey. PloS one. 2011; 6(5): e20331.
- Ng M, Freeman MK, Fleming TD, et al. Smoking prevalence and cigarette consumption in 187 countries, 1980-2012. JAMA. 2014; 311(2): 183-92.
- Kulkarni RR, Kumar Y, Patil S. Prevalence of geriatric tobacco use in an urban slum of Belagavi, Karnataka. International Journal of Advanced Community Medicine 2019; 2(1): 01-04.
- Mini GK, Sarma PS, Thankappan KR. Pattern of tobacco use and its correlates among older adults in India. Asian Pacific Journal of Cancer Prevention. 2014; 15(15): 6195-8.
- National Family Health Survey (NFHS-5) 2019-21. Available at: URL: https://dhsprogram.com/pubs/pdf/FR375/FR375.pdf. Accessed 11 June, 2024.
- Patil AP, Khona PP, Patil M. Prevalence of tobacco consumption in an urban area Belgaum, Karnataka, India. Int J Community Med Public Health. 2016; 3(11): 3059-62.
- Mini GK, Sarma PS, Thankappan KR. Pattern of tobacco use and its correlates among older adults in India. Asian Pacific Journal of Cancer Prevention. 2014; 15(15): 6195-8.
- World Health Organization. Global Report on Trends in Prevalence of Tobacco Smoking. Geneva: World Health Organization; 2015. Available at: URL: https://www.who.int/tobacco/global_report/en/
- Maheshwari V, Sodhi B, Sharma R, et al. Determinants of tobacco use patterns and predictors of quit among older women in India: Findings from the study on global aging and adult health. Pneumon. 2024; 37(1): 1.
- Rani M, Bonu S, Jha P, et al. Tobacco use in India: prevalence and predictors of smoking and chewing in a national cross sectional household survey. Tobacco control. 2003; 12(4).
- Sukumar GM, Banandur P, Dagar V, et al. Prevalence and factors associated with tobacco use among beneficiaries attending the youth mental health promotion clinics (Yuvaspandana Kendra) in India: A case-record analysis. Tobacco Prevention & Cessation. 2022; 8.
- Viswanathan A, Doddamani A, Praharaj SK, et al. Substance Use Among People Seeking Health Care Services in Primary Health Care Settings in Coastal Karnataka. Indian Journal of Psychological Medicine. 2024; 46(6).
- Nichter M, Nichter M, Carkoglu A. The Tobacco Etiology Research Network. Reconsidering stress and smoking: a qualitative study among college students. Tob Control. 2007; 16(3): 211-214.
- Sreedevi A, Majumdar A, Olando Y, et al. Experiences and Beliefs on Tobacco Use, Cessation in India: A Qualitative Study. Global Heart. 2023; 18(1).
- Gupta R, Pednekar MS, Kumar R, et al. Tobacco cessation in India–Current status, challenges, barriers and solutions. Indian Journal of Tuberculosis. 2021; 68: S80-5.
- Chockalingam K, Vedhachalam C, Rangasamy S, et al. Prevalence of tobacco use in urban, semi urban and rural areas in and around Chennai City, India. PLoS One. 2013; 8(10): e76005.
- Ahammed B, Maniruzzaman M, Kundu S, et al. Prevalence and risk factors associated with tobacco smoking among adults in India: a nationally representative household survey. Family Medicine & Primary Care Review. 2019; 21(4): 307-17.
- Deshmukh S, Ghooli S, Kurle RS. Knowledge, attitude and practice of gutkha chewing among youth in Hiroli village of Kalaburagi district. Int J Community Med Public Health. 2019; 6: 1324-8.
- Ahammed T, Ahmed NU, Uddin MJ. Changes in prevalence, and factors associated with tobacco use among Bangladeshi school students: evidence from two nationally representative surveys. BMC Public Health. 2021; 21: 1-3.
- Giriraj B, Dhage A. Prevalence and Characteristics of Cigarette Smoking Among Adults in Urban Community in Gulbarga. Sch. J. App. Med. Sci. 2015; 3(4B): 1752-1755.
Review: Research |
Subject:
Public Health
Received: 2025/02/17 | Accepted: 2025/07/16 | Published: 2025/01/12
Received: 2025/02/17 | Accepted: 2025/07/16 | Published: 2025/01/12
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution 4.0 International License. |
